
These days, it seems there is an anti-EMR proclamation to match every anti-vaccination decree. As the old adage goes, “You can lead a horse to water, but you cannot make it drink.” For the skeptics, by the end of this article, hopefully the water will reveal itself to be a little more palatable.
Paper vs Basic EMR vs Advanced EMR:
In its most basic form, EMR is used simply as an electronic typewriter and appointment scheduler. As a next step in advancement, the EMR user takes advantage of features like prescription writers, some basic note templates for common types of visits, and perhaps using a few simple “reminders” to aid in patient care. This would be classified as “Basic” EMR use. “Advanced” use of EMR includes taking advantage of features such as searches, complex reminders, and many of the other innovative features that EMR systems have to offer.
Even in its most basic form, EMR transcends paper charts in arguably every way imaginable.
EMR has become a Scapegoat:
Critics of EMR often claim that much of their day is spent entering data into a computer, rather than face to face patient care. They are frustrated and feel this type of administrative work is a waste of valuable physician time and expertise. This is all totally understandable and merits improvement. However, EMR is not to blame here. EMR is simply the tangible instrument for the deeper issues and causes here.
It is not the EMR that is causing nor necessitating the diversion of physician time. Rather, it is the increasingly burdensome administrative requirements of today’s clinical practice. It is the CPSO and MOHLTC requirements that mandate thorough documentation. It is the mounting complexity of each and every patient, compounded by a growing number of clinical practice guidelines for each of their chronic conditions. It is the incentives and corresponding metrics that amplify administrative burden. It is government and hospital policies that mandate documentation requirements.
Whether or not each of these factors is misguided is beyond the scope and purpose of this article. The fact remains, though, that the digression in clinician time is due to factors like these, and not because the EMR is somehow demanding the clinician’s time.
EMR is not the problem here. It is the solution. The administrative burden caused by all of the above factors would undoubtedly be even more time consuming and inefficient if not for EMRs.
One Click is Faster than Fifty Keystrokes:
Even in its most basic form, EMR as a word processor with elementary templates for notes is exponentially more efficient than hand-written paper charts – not to mention the legibility factor.
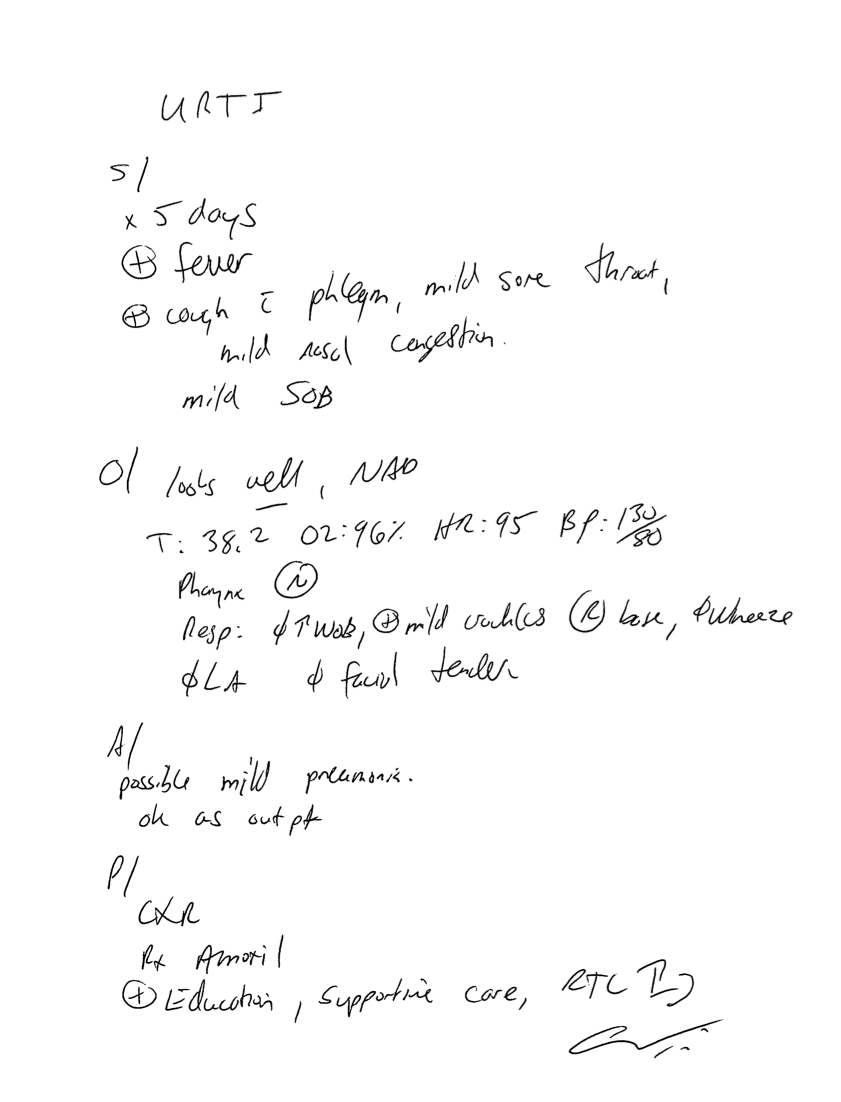
Imagine a patient who presents with a respiratory infection. Assessment reveals clinical suspicion of pneumonia. A chest x-ray is ordered and the patient is prescribed amoxicillin. Ultimately, the physician will need to document a chart note, complete an x-ray requisition, and write a prescription.
The chart note may look something like this, and took 2:26 minutes to write:
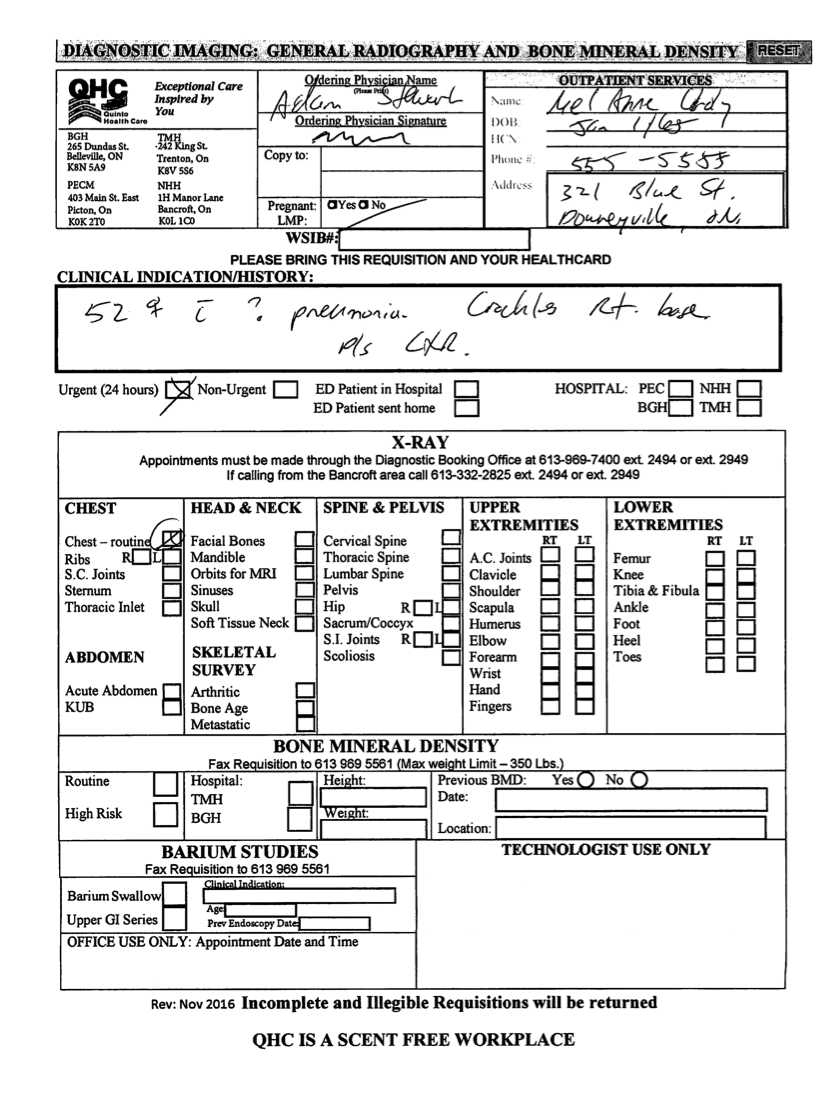
The hand-written chest x-ray requisition may look something like this, and took 1:11 minutes to write (not including the time it would have taken to manually retrieve the paper requisition):
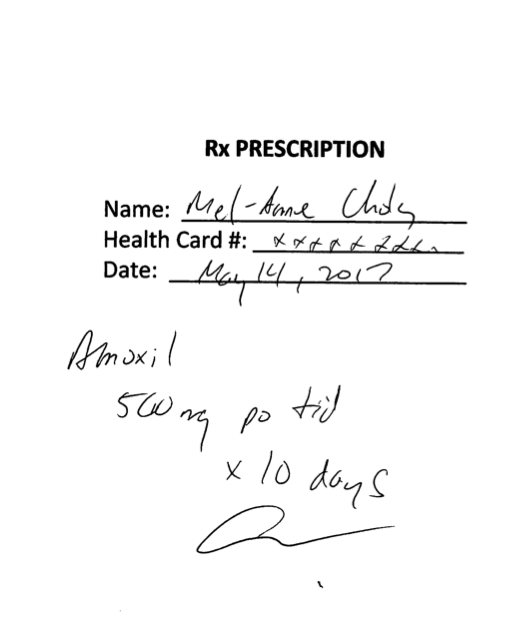
The hand-written prescription may look something like this, which took 43 seconds to write:
This paper-based encounter took a total of 4:20 minutes in paper-work.
In comparison, using an EMR with just basic features, the same encounter required a total of only 1:37 minutes to write the chart note (1:05 minutes), prepare the x-ray requisition (29 seconds), and write the prescription (13 seconds).
Here, basic EMR use saved 2:43 minutes in administrative and charting time in this simple visit example. This is not to mention all of the time saved in chart retrieval and filing, the administrative time saved by electronically faxing the prescription and requisition, and the added efficiency of tracking a pending test result.
If one assumes an average time savings of even 3 minutes per visit, multiplied by 100 patient visits per week, that amounts to 5 hours of physician time saved each week, in just this simple example.
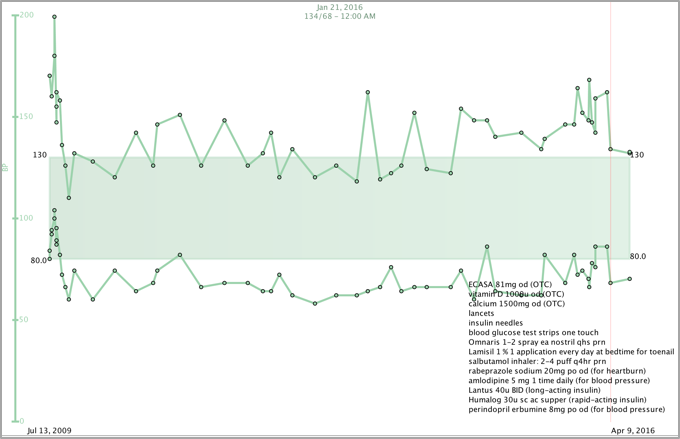
In actual practice, the efficiency savings are even greater when one considers the difference in time saved with more complex visits such as chronic disease management, like diabetes flowsheets, and so on. For instance, EMRs allow easy graphing of measurements such as blood pressures, weights, and A1C levels, so as to have this type of data readily available within a couple of key strokes, thereby improving the ease and quality of clinical decision making.
Metrics and Population Health Management:
There are deserved merits and criticisms for most of the popular metrics that physicians are asked to track, and the incentives that are sometimes tied to them. These types of discussions are beyond the purpose and scope of this article.
That aside, the benefits of screening for cervical cancer in women are relatively non- controversial. Imagine, for example, a family practice that has 600 applicable women who are to be screened every three years with a PAP smear. Using an EMR, a simple search takes just a minute or two to generate a recall list. With advanced features such as bulk emailing, hundreds of women can be notified and recalled using less than ten minutes of a staff time. Whereas with paper charts, the amount of administrative burden required to find and recall every single woman who is overdue for her PAP smear is enormous, not to mention subject to a tremendous amount of human error and inaccuracy.
Magnify this example by the similar administrative burden (or savings with EMR) of recalling patients for the multitude of other tests they require (Colon Cancer screening, Mammograms, Immunizations, Blood Pressures, certain blood tests, Bone Density Tests, etc). There is simply no logical justification for the use of paper charts over EMR, neither in terms of efficiency nor quality of patient care.
Other EMR Advantages:
EMRs carry other sorts of advantages that paper charts cannot offer, including but not limited to:
– Legibility
– Accessibility (i.e. remotely from outside of clinic)
– Safety checks such as drug interaction warnings
– Intra-office messaging features
– Efficiency of sending referrals (that are high quality and comprehensive)
– Ease of ability to track pending tests and referrals
– Ease and potential for data retrieval and analytics
Even its most basic form, the immediate and tangible advantages that EMR offers over paper charts are clear. This is not to mention the spectrum of advanced capabilities not explored within this article. EMR should not be a scapegoat. Frustrations with current administrative burden should be more appropriately directed at its more insidious root causes. If anything, EMR and technology will continue to assist as solutions, rather than be obstructions.
– Dr. Adam Stewart
May 14, 2017